Ibogaine, of all things
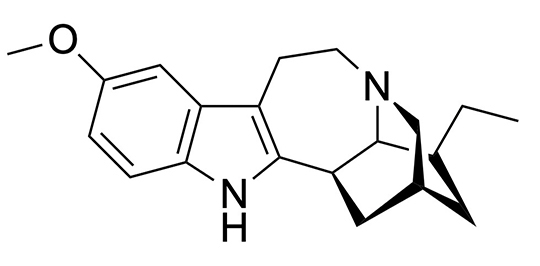
IBOGAINE MOLECULE’S unique structure allows the interaction with multiple neurotransmitter systems simultaneously.
One of the many unexpected political happenings this spring involved our country’s administration signing an executive order aimed at increasing the review of ibogaine and other psychedelic drugs to treat various mental health conditions. When I was in college, I worked in an organic chemistry lab for four years researching novel psychedelic compounds, and one of our leading projects was an investigation of ibogaine and its medicinal properties, so this was particularly attention-grabbing for me. There is something disorienting and surreal about some of the country’s most traditionally minded individuals championing research on a ceremonial African psychoactive shrub, though the framing around veteran care makes the shift easier to understand. Let me break these ideas down a bit.
 Ibogaine is a psychoactive alkaloid produced by the root bark of the perennial rainforest shrub Tabernanthe iboga, indigenous to West Central Africa. It can induce a powerful and long-lasting (24 to 72 hour) experience known for psychoactive effects that are characteristically oneirogenic (dreamlike). The root of this iboga tree has been used for centuries by Indigenous groups—most notably the Bwiti religion in initiation rites, social rituals and bonding—for induction of visionary states, to communicate with ancestors, and as a traditional medicine.
Ibogaine is a psychoactive alkaloid produced by the root bark of the perennial rainforest shrub Tabernanthe iboga, indigenous to West Central Africa. It can induce a powerful and long-lasting (24 to 72 hour) experience known for psychoactive effects that are characteristically oneirogenic (dreamlike). The root of this iboga tree has been used for centuries by Indigenous groups—most notably the Bwiti religion in initiation rites, social rituals and bonding—for induction of visionary states, to communicate with ancestors, and as a traditional medicine.
In the 20th century, ibogaine was recognized as a powerful medicine for treating substance use disorders through underground research and experimentation. This research showed that just a few experiences with ibogaine could have long-lasting effects in reducing drug use as well as significant reductions in acute withdrawal symptoms. These promising observations are complicated by the fact that one of the many targets of ibogaine and its primary metabolite noribogaine, is the hERG potassium channel. Ibogaine blocks this ion channel, which results in QT prolongation (which is when the heart ventricles take too long to recharge between beats) and possible fatal cardiac arrhythmias. In other words, there is a concerning cardiac risk with ibogaine. Certain research groups, like the one I used to work in as a student (Sames Group at Columbia University) are making significant advances in tailoring the drug using medicinal chemistry, so it keeps its therapeutic properties but does not have any adverse cardiac effects.
In addition to its efficacy in treating substance use disorders, more recent research has pointed to ibogaine’s potential to treat trauma-related psychological and cognitive impairment. The population supporting these findings are a group of U.S. veterans who sought psychedelic treatment at a clinical program in Mexico. Another recent study completed at Stanford University suggested ibogaine (co-administered with magnesium to offset the adverse cardiac effects) has significant potential to treat PTSD and mild traumatic brain (mTBI) in veterans.
My friend Hamilton Morris who is a journalist, chemist, and expert on these topics said, “I understand why some people are concerned about anything coming from the current administration, but I think it’s a good thing that will facilitate research and accelerate clinical development.”
The story with ibogaine suggests we may need complex drugs to treat complex conditions. The clinical results hold a lot of promise and hope for those in need. As research continues, our challenge will be how we responsibly study, potentially use, and administer a substance that exists at a juncture of science, culture, history, and experience. I presume some interesting developments will happen.
Questions? Comments? Email pcd1130@gmail.com.
Category: News